
Why the Public Always Loses in “Public / Private Partnerships” — Part 1
Why the Public Always Loses in “Public / Private Partnerships” — Part 1
Why I’m not “Vaccinated” — Part 1 on the failures of Big Everything

I can’t believe I have to add this, but such is the times we live in. I am not a doctor. This is not medical advice. This is how, and why, I made the personal medical decision I made, and the data that supports that personal medical decision. As with everything I write, the data is what the data is, how we interpret it, and use it (or don’t use it) to make decisions, is what makes us a free people.
As with most questions in life, there’s a simple answer to why I’m not “vaccinated,” and a complicated answer. The simple answer to the simple question is that I don’t take medicine I don’t need, and I don’t need to take a shot to “prevent” (or treat) covid. I’m young, I’m healthy, and covid is of zero risk to me1. I’m sure most people read that last statement and gasped with horror. How could I possibly say it’s of zero risk to me, have I not heard ALL THESE HORROR STORIES!? Well, if you’ve read me before you know I don’t care about your horror stories, I care about the data. And here’s the data:
Despite “the worst pandemic in 100 years” the all-cause mortality trend, summarized across all of western and northern Europe, for people in my age range, continued to DECLINE going into 2021. If you look closely, you’ll notice a spike in March of 2020, you may also notice that spike is still lower than the normal flu season spike in 2018. You’ll also notice these “spikes” represent an additional 100 deaths, across a population of tens of millions of people. If you look even closer, you might notice that downward trend officially started to change as we entered the “vaccine era” in 2021 … but we’re not quite to that part of the story yet:
https://www.euromomo.eu/graphs-and-maps
The simple answer is simple — I don’t take medicine I don’t need, and I very much don’t need this medicine. The complicated answer, on the other hand, gets more complicated every day.
I want to get infected…
In May of 2020 I wrote an article titled “Micro Solutions are Creating Macro Problems” Near the end I argued that 1. There is very, very clear evidence, going back decades, and literally litigated in court in Canada, that masks, even in hospital settings, have no impact on the spread of aerosolized viruses, and 2. That even if they did reduce spread, you shouldn’t want me to wear one. The logic was relatively straightforward. The only way an actual pandemic ends is by the community in question reaching herd immunity. That is, a large enough portion of the population has developed immunity to the pathogen such that R (how many people a carrier infects, on average) falls below 1, and the pandemic burns out. With endemic viruses like coronaviruses this is irrelevant, we just live alongside them as we have for literally tens of thousands of years (coronaviruses existed before humans did and they’ll exist after humans are long gone), but we were (are?) still pretending this is a pandemic, so pandemic rules we shall apply.
“15 days to slow the spread” was the official rallying cry. As I argued at the time, the existing CDC pandemic framework (this was from back before the CDC and NIH decided rent reform, and Time Magazine covers, were more important than studying infectious diseases) didn’t qualify covid-19 as a pandemic, but if we needed 15 days to add protection in hospitals and nursing homes, so be it. Closing schools was madness, telling people not to go outside was less detrimental, but even more ridiculous, and so it was very clear, very early on, that our highly politicized “public health” establishment was playing a political game and not a medical one, and that scientists had been sidelined and replaced by “scientists.” Either way, we’d shutter for 15 days, put in place the needed recommendations for those at high-risk, and then we’d move on.
Only, we never moved on. We pretended masks could slow the spread (they can’t) and that social distancing would also help (it did, a little), and then… Well, there never was a clear “and then.” Why are we slowing the spread? I can’t imagine we just wanted to drag this thing out, though honestly who knows. For a little while we pretended it was to spare hospitals, but no hospitals, anywhere in this country, were ever anywhere near being overwhelmed, so they had to give up that farce relatively quickly (remember that giant empty naval ship in the NYC Harbor? Probably not, they kind of worm holed that whole disaster). So, why were we continuing the masks and the distancing and all the theatre? As far as I could tell we were no longer even pretending there was a reason, we appeared to just be doing it to do it (yes, I just described 99.9% of US politics, but bear with me). So where else could I look to figure out what the heck was going on?
I looked northeast, and thankfully, as always with covid, we had the Swedes. And they were actually executing the traditional pandemic framework that had been developed over decades specifically to respond to situations like we found ourselves in; implement risk specific recommendations, often age based and relative to the severity of the threat, and then… Well, we can’t protect elderly people forever, or segregate them from society forever, or keep them from their loved ones forever, so, what’s next? Here in the US, we were just spinning. There was no “what’s next.” It was mitigation for mitigation’s sake. But in Sweden they used the whole framework, not just the “forever to slow the spread” opening paragraph our politicians added to the framework (when they literally erased the framework, by removing it from the CDC website) in May of 2020.
Once the high-risk were protected (and remember, prior to “political crisis 2020” high-risk was an opt in process — if you think you’re high risk, you opt-in to the recommendations, and if you don’t, even if you are, you don’t… that’s what free will is) you let everyone get on with life in hopes the virus moves through the rest of the community as quickly as possible 2. The faster it moves, the less disruption for society, and the sooner everyone, including the high-risk, can get on with life. This is the fundamental principle of “chicken pox parties,” something all of us understood and most of us participated in, and the basis for all pandemic response frameworks ever developed: provide recommendations based on severity and risk profiles, create enough time to spread the message and allow people to take the recommended precautions, and then allow the healthy to move on with life. And the Swedish executed it.
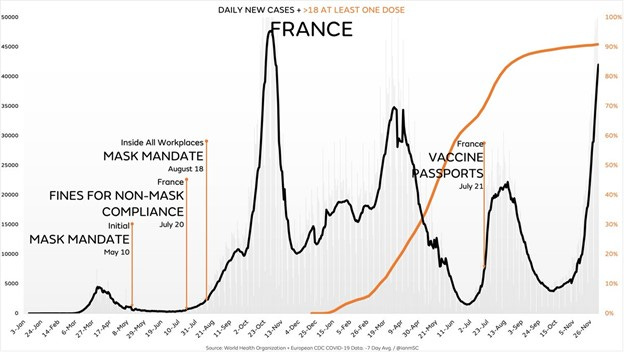
As countries around the world are doubling down on vax mandates, strict lockdowns, and masks (good lord) as their cases skyrocket — here’s France — almost 90% “vaxxed,” and vax passport restrictions, for reference:
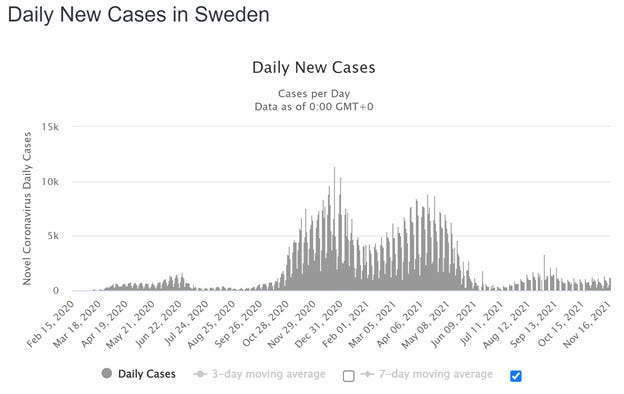
Sweden let it sweep through their young population, the VAST majority of whom never even knew they had it and moved on with life. Here is Sweden, for reference:
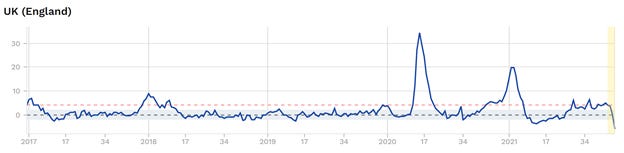
And, with zero restrictions in place, here is the all-cause mortality change for 45–64 year old Swedish citizens. The all-cause in younger age groups is even more irrelevant. They let covid fly through their population and were exactly zero worse for the wear because of it:

The above chart shows mortality trends over time, by plotting the z-score of the weekly total mortality. Z-score is a statistical mechanism for evaluating changes against the base rate. The grey dotted line is the base rate mortality, the blue is a single standard deviation, and the red dotted line shows 2 standard deviations from the base rate. All this data, for all countries that report, are available at https://www.euromomo.eu/graphs-and-maps
Naturally your question should be, sure, 65 and under may not have been impacted, but surely overall all-cause mortality increased SIGNIFICANTLY given the “worst pandemic in 100 years.” Well, about that:
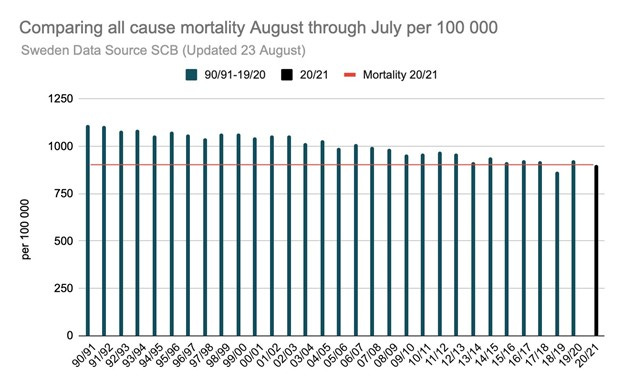
Turns out the mortality rate, for all of Sweden, and this is NON-AGE ADJUSTED, continued to decline through 19/20 and 20/21 as well. I’ll leave this here for you to do with what you wish, but just keep in mind that the “worst pandemic in 100 years” lead to Sweden having its second and fifth LOWEST mortality in the last 30 years.
Now, I can’t force my country, or my state, to take the Swedish model (though Michigan eventually was forced to through this beautiful thing called democracy, so at least we’re trying…) but I could do my part.
As already stated, I’m not at risk from covid, so dive right in was always my plan. I want to get covid as fast as I can, kick it, and become a break in the chain.
And so that’s what we did. We lived our lives as perfectly normal as we could. And, eventually, way later than we had figured, we got covid. Once we had it, we hung around the house, all four of us got it together. The kids kicked it in about 15 minutes, my wife and I had shitty colds for a week, and on went life no different than it was before. It was a shitty cold, no doubt, but not even in the 3 worst colds I’ve had as an adult (weird thing to remember, I know, but I literally fell asleep taking my GMAT I had such a bad cold, and I was stuck in a hotel room in LA for three days in October of 19 I had such a bad cold, so they weren’t that hard to recall …). Of the 15 other people that got it the same time we did (12 of whom were vaccinated), my symptoms were somewhere in the middle, and even that was mostly because I got it during a giant golf tournament where I was, let’s say, not taking great care of my body.
And Natural Immunity Works… because all immunity is Natural
And now I have natural immunity 3. Is it perfect? Of course not, it can’t be. As we’ll discuss, coronaviruses mutate too quickly for our body to ever stay fully ahead of them. This is why most people who get bad colds/flu (that is, are susceptible to coronaviruses generally, which is not all of us. Just as I can get poison ivy from looking at it and my wife can roll around in it and never know the difference, so bodies respond differently to coronaviruses) generally get one about once every four years as an adult (the younger you are the more frequently you get them — if you have kids you know this — because your breadth of immune response is smaller, but your immune system is stronger, so you fight it off quicker and easier, but develop a less broad immune response because of how “easily” you beat it). Given how quickly coronaviruses mutate that’s about how long it takes, on average, for the mutations to cause a viral strand unique enough to beat, at least short term, your existing T-cell reconfiguration and antibody development. Then you kick it again, and start the cycle all over again, this time with even more robust, and durable, immunity.
But think about this logically, and not exclusively in the case of covid-19 “vaccines,” but all vaccines. If the goal of the vaccine is to trigger an immune response, then an ACTUAL immune response will always be more robust. With highly stable viruses (coronaviruses are exactly the opposite of that) the vaccine is an almost exact mirror of the actual virus, but in a lower dose and using “sick” viruses that will not replicate as quickly, which makes it easier for the immune system to win. But in EVERY case, it is always your natural immune response that protects you — either more completely by beating the active live virus, or more simplified by beating a tired virus that was medically induced 4.
Despite all the “success” of vaccines, this is why we have eradicated exactly one virus ever. Because it is very, very hard 5. The medicine only triggers the natural immune response. And again, just like our pandemic response framework, we’ve known for literally a century that natural immunity is more robust and complete, against all viruses, than medically induced immunity. This difference is the most critical reason why we’ve never, not ever, vaccinated people who had recovered from a disease — until 2021 that is… because, well, of course****
Given the above, at least for the next couple of years, my family is now a break in the chain (and we’ll keep becoming one every time society freaks out about a virus that led to an all-cause mortality DECREASE in countries that didn’t lock people out of hospitals and encourage them to Lysol their groceries).
So, when kids at school get covid, symptom free of course, because they’re kids, and they aren’t allowed to do anything, they can come play at our house. Because we’re already breaks in the chain, and that’s a great place to be. That’s why I didn’t get the “vaccine,” because I’d rather my immune system respond the old fashion way than fake it through a medicine I don’t need. And respond the old-fashioned way it did — we kicked the virus, we have the antibodies (proven through testing), perhaps more importantly we’ve developed T-cell responses so fighting future coronaviruses will be easier as well, and now we’re a healthy, happy family that also acts as a break in the connective chain of viral replication. It hits us, it doesn’t replicate, we don’t get sick or spread the virus, and others are better off because of it. We are now a part of the herd, that’s pushing toward herd immunity.
This is how fighting disease has always worked, or at least always worked until early 2021 when a community that had already lost its collective mind literally stepped off the cliff.
But even that doesn’t tell the whole story, so we should probably start at the beginning. And the beginning is…
A “vaccine” in name only
You can’t vaccinate against coronaviruses. You can “vaccinate” against them, apparently, but you can’t vaccinate against them. We’ve known this for decades. We tried against MERS and failed, we tried again against SARS and failed, they asked Merck to participate in Operation Warp Speed (what a joke) and they said “can’t be done” 6, and yet, here we sit. You cannot vaccinate against a coronavirus — they mutate too quickly, their “flight” response in the biological battle over fight or flight is too strong, and they have too many different mechanisms for contact and replication to vaccinate against them. And we know this.
We knew this when Trump was president (and being hoodwinked by the medical establishment), and we know it now under the Biden administration who, let’s be honest, doesn’t even know what’s going on. The only thing better than listening to all the people scream they would never “TAKE A VACCINE THAT TRUMP CREATED” is listening to them now scream that they “CAN’T BELIEVE ALL THESE TRUMPERS WON’T TAKE A PERFECTLY SAFE AND EFFECTIVELY AND SAFE AND EFFECTIVE VACCINE THAT’S FREE AND SAFE AND EFFECTIVELY EFFECTIVE.” It’s actually hard to always be wrong — but we’re turning it into an art form.
So, if you can’t vaccinate against a coronavirus, but we created, and sold, to the tune of billions of dollars, a “vaccine,” what exactly is a “vaccine” anyway?
And that’s where today’s contradiction comes into play. Cause the truth is, we don’t know. The CDC is so confused by what this “vaccine” is they literally changed the definition of vaccine to replace the word “immunize” (the actual point of a vaccine) to “protect” (which, of course, doesn’t have a technical definition). The old contradiction between the “vaccine” being the tool of the devil when Trump was in office and now being manna from heaven while Biden is in office we can laugh at. It’s political, and we expect irrationality when it comes to politics. Today’s contradiction, on the other hand, is a bit more concerning, given the millions of doses of these “vaccines” we’ve given, and the “FDA approval” one of them will soon carry.
When the “vaccine” results were first released it was a miracle drug that “reduced the likelihood of mild to moderate COVID by 90+%.” You remember those days… we all heard the announcements, we all whooped with joy (well, not all of us) and we were all so happy that we had found this miracle drug whose clinical trial proved that it reduced the spread of covid. Except, the wording was all very weird, and no one had answered the question of why we needed a vaccine for a virus that, as previously stated, wasn’t, on its own, increasing mortality rates, to begin with, so I was skeptical. And I never trust anything the media reports, and I probably trust big pharma even less than the media, so, I did what I always do — I annoyed my wife. I told her the statement didn’t make any sense and dragged on and on and on until she inevitably just walked away. And then I really annoyed my wife and went and read the study abstract itself. I’m going to guess you haven’t read it (If you have, that’s awesome, but in my life, and I talk about this a lot, I think I know one other person who has actually read it), so here it is:
https://www.medrxiv.org/content/10.1101/2021.07.28.21261159v1.supplementary-material — just click on “supplementary appendix” at the top of the article.
The full text can be found here — https://www.medrxiv.org/content/10.1101/2021.07.28.21261159v1.full-text if you’re interested in going deeper.
There are a lot of odd things about this, for instance, the median age of death with covid-19 is ~80 years of age, yet less than 4% of the total evaluated population is over 75. But the most interesting oddity was that they didn’t test people as part of the trial. You can’t walk into a gas station and not see free covid testing available. They are EVERYWHERE. And yet, in a trial for a VACCINE (that is, something that should prevent you from getting a disease) they did not do daily, or weekly, or even monthly testing of the participants to see if they were actually protected from getting the virus. And remember, the point of a vaccine is to eradicate a virus. If people are still getting it, even if they aren’t showing symptoms (as was the case for the vast majority of people before this “vaccine” existed) then the virus is continuing to circulate and the “vaccine” isn’t serving the purpose of a vaccine; it’s a treatment at best, and a giant bag of risk with no benefit, at worst.
What they chose, instead of required testing, was to “monitor symptoms,” and to only qualify a covid-19 case as a “case” if the person BOTH tested positive AND had symptoms. Does that sound unusual to you? Because it should. It should INFURIATE you, if you’ve been paying attention. EVERYONE, from sports teams to college students, and nurses to meat plant workers, have been tested, AND TREATED AS DANGEROUS AND FORCED TO QUARANTINE IF THEY TESTED POSITIVE REGARDLESS OF SYMPTOM DISPLAY. We had entire college basketball games cancelled without a single symptomatic case, and yet the drug trial positioned as a “cure” to the pandemic requires symptoms!?!?!?!
If I’m running a trial for a vaccine intended for global distribution to fight a “pandemic,” I’m pretty sure I’m going to test everyone, very frequently, to understand the actual impact on the spread of the freaking virus. For the last 18 months we’ve CONSTANTLY been harped on about “asymptomatic spread” (something that doesn’t exist) as the justification for requiring masks and social distancing, but now, in the actual drug trial, we’re saying you’re only “sick” if you’re actually sick, and that “asymptomatic” is no longer a thing to even consider? If I wasn’t so angry about this, I’d think it was a joke.
This should bother you. Regardless of your political bent, you must admit your medical/media establishment have been lying to you the entire time, one way or the other. Either “having the virus” (regardless of symptom display) is the problem — as it has been treated for the last 18 months, or actually being sick is the problem — as it should have been treated for the last 18 months, but it can’t be “having the virus” when we’re talking about playing college basketball (with kids who are at zero risk from COVID) but being actually sick when we’re talking about testing for a vaccine. I realize that politics is defined by having it both ways, but science isn’t. We literally applied stricter standards to attending a college class than we did to a drug trial for the m**** f**ing “cure” to our epidemic.
In my first draft of this piece, I called these trial design errors sophomoric. But they aren’t. That would be to conclude that these were mistakes… and after reading the trial, and analyzing the public messaging a few dozen more times, that’s just impossible. These weren’t mistakes. They were intentional in design, and they were specifically because Pfizer already knew the “vaccine” wasn’t a vaccine.
I was discussing this with a scientist friend of a mine (a tenured professor at an, unfortunately, very prestigious university (she’ll get the joke)) and used the analogy that these “vaccines” are closer to steroids than they are to a vaccine. She hated that analogy, because she was looking at it scientifically rather than metaphorically — because she’s smarter than me. And scientifically she’s obviously right — these are gene therapies that we have zero understanding of. Steroids we understand. That said, I still think as a metaphor the comparison makes sense.
If you know anything about anabolic steroids, you know they work. They will absolutely make you stronger. There are just two issues with them — while you’re taking them, they mess you up, and once you stop taking them, they really mess you up. They are artificially increasing your ability to build muscle (these “vaccines” artificially increase your ability to fight off covid symptoms) while you’re taking them, only continued dosing is extremely dangerous to every other function of your body (kidneys, liver, heart, etc…) and once you stop taking them, you’ve messed up your natural ability to build muscle so significantly that you are, for sure, going to end up worse off than you started.
The exact same is true here… but we’ll get to the “worse off than you started” part of the analysis in a minute.
Just like steroids, what the study did “show” (ignoring all the errors in study design for the minute) is that the “vaccine” did reduce mild to moderate covid-19 symptoms. In steroid terms, it built muscle, just like it said it would. To the tune of 90% of effectiveness (81 covid “cases” in the treatment group, and 873 “cases” in the placebo group) post dose 2 (data summarized in the “Efficacy” section of the report, found at https://www.medrxiv.org/content/10.1101/2021.07.28.21261159v1.full-text)
But today, we know for sure the vaccine does not reduce mild to moderate covid by 90+%. Today we laugh when someone has a “breakthrough” case. Basically everyone you know got “vaccinated,” and more and more and more of them are getting covid, to the point where it isn’t a breakthrough, the vaccine’s simply don’t stop you from getting, or spreading, covid. This is widely accepted at this point, even if you personally continue to grasp at straws (again, see Austria, or Vermont, or the UK, or anywhere else with astronomically high vaccination rates that also have astronomically high covid rates). Here is the chart, published this week (and every week) from the UK, which shows covid positivity rates, hospitalizations, and deaths by vax status:
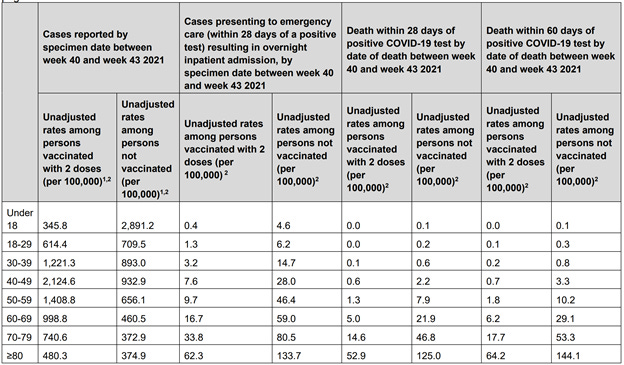
The far left of the chart is rates (not raw numbers, but rates per 100,000 individuals) for covid positivity. As this chart clearly shows, in every age category over 29, you are not only more likely to get covid, but you are substantially more likely to get covid, if you are “vaccinated.” Like in some cases 2–3x more likely to get covid.
And, hilariously, the trial itself could have predicted this. The trial was, VERY specifically, ended at exactly 6 months, and then the placebo arm of the trial was immediately “vaccinated.” Again, not sophomoric (you NEVER screw up the placebo arm in a trial — generally the placebo arm remains that way for many, many years. How else would you gather comparative data???), but intentional. They did this, because as they note themselves, they could already see that the effectiveness of the “vaccine” was waning over time. Here is the exact passage:
“Efficacy peaked at 96.2% during the interval from 7 days to <2 months post-dose 2, and declined gradually to 83.7% from 4 months post-dose 2 to the data cut-off, an average decline of ∼6% every 2 months. Ongoing follow-up is needed to understand persistence of the vaccine effect over time, the need for booster dosing, and timing of such a dose. Most participants who initially received placebo have now been immunized with BNT162b2, ending the placebo-controlled part of the study. Nevertheless, ongoing observation of participants through up to 2 years in this study, together with real-world effectiveness data,14–17 will determine whether a booster is likely to be beneficial after a longer interval. Booster trials to evaluate safety and immunogenicity of BNT162b2 are underway to prepare for this possibility.”
They already knew this was, in no way, a vaccine. They were pretending it was a linear decline in effectiveness (of course not) as opposed to “half-life” decline (like all other molecules known to man), and then erasing the data so it couldn’t be proven. Of course, being the businessmen (and not scientists) that they are, they used this opportunity to ALREADY START ARGUING FOR BOOSTERS. That’s right, in a trial for a VACCINE (something that should last a lifetime), they were already arguing for why their drug was amazing, obviously, but would require you to keep buying and taking it every 6 months, forever, to “protect” against a virus that greater than 99% of the population doesn’t need protection from. You literally can’t make this shit up.
There’s also the issue of “original antigenic sin” 7 which argues that “vaccinating” mid-pandemic actually decreases the body’s ability to respond to the inevitable viral mutations that will occur naturally, and likely also helps explain why we’re seeing total “vaccine” failure, at a societal level, when analyzing viral spread.
Okay, so it was a bad trial design (or a genius trial design depending on whether you care about health or money) but, you say, the above data is very clear that it does significantly reduce hospitalizations and deaths. And, as you can see, the data found in these analyses support that claim 8.
A vial of “protection?”
… but the actual Random Control Trials, used to justify the Emergency Use Authorization (“EUA”) for these “vaccines” in the first place, show exactly the opposite. There is a reason why Pfizer and Moderna never claimed to reduce hospitalization and death — only “mild to moderate covid” 9… those numbers are VERY hard to game in a trial. You can very easily call one person’s sneeze allergies and one person’s sneeze covid. A person showing up at a hospital is a person showing up at a hospital, and someone dying is VERY hard to hide (though they tried…).
In the only trial completed and shared to justify the EUA, and eventual FDA approval, of the covid “vaccines,” there were, reported at the time, 29 deaths. 15 in the vaccine arm and 14 in the placebo arm. Of course, some of those 14 deaths in the control arm were blamed on covid, and NONE of the vaccination deaths were blamed on the vaccine. But the data is what the data is, and so arguing it reduces the risk of death would be very hard. Not impossible, and they tried, but 15 is greater than 14, so… Even more outlandish, in the entire study, across both placebo and treatment, there were 31 TOTAL “severe” covid cases in the entire 44,000+ study population. Based on this study, doing nothing is 95% percent effective against getting covid in the first place (roughly 860 out of 23,000 placebo recipients got covid-19) and doing nothing is 98.5% effective against not getting severe covid (30 out of 23,000). And this study was used to justify global “vaccine” rollout, “vaccine” mandates, and even FDA approval. Kind of interesting right?
All this considered, Pfizer clearly couldn’t say the “vaccine” reduced deaths, but what about hospitalizations? There were only 31 “severe” covid cases recorded in the entire trial, and they skewed VERY heavily toward the placebo arm (30 to 1), so it worked, right? Well, hospitalizations actually look just like deaths. If you look ONLY at severe outcomes “caused” by covid (however they define that) then yes, it looked like it worked. But take a step back and what do you see? When looking across the entire study there were 137 “severe serious adverse events” from all causes across the study. 71 of these “severe adverse events” were in the “vaccination” arm and 66 in the placebo arm. So, again, the data clearly says the “vaccine” also doesn’t reduce the risk of severe adverse events. In fact, just like with deaths, a cursory glance would say it actually increases the likelihood of having a critical care issue. So great news, you’re protected against “severe” covid, whatever that is, but more likely to be hospitalized if you take the “vaccine,” than if you don’t. This is one interesting “medicine.”
So, to summarize, we ran a giant drug trial to justify the expenditure of billions and billions of dollars and untold human capital to prevent a disease you have less than a 5% chance of contracting in the first place, and an almost immeasurably small risk of having a severe illness from (0 is within the confidence interval for your likelihood of getting “severe” covid as part of this study) and we left with these takeaways:
Covid is extremely, extremely rare (it isn’t, which is why they should have re-run the trial and ACTUALLY TESTED PEOPLE)
You are as likely to die from all-causes as you are to get severe covid, regardless of “vaccination” status
You are more likely (though not statistically significantly more likely) to die if you take the “vaccine” than if you don’t
You are more likely to have a severe adverse event if you take the “vaccine” than if you don’t
We have an insanely corrupt medical infrastructure that immediately authorized these “vaccines”
But that can’t be the end of the story, because how did the trial get everything wrong? How did the trial manage to show that the “vaccine” reduced covid, but didn’t reduce hospitalizations and death, and yet societal data shows it encourages covid but may reduce hospitalizations and death?
Like most things, I tend toward the simple answer. And the simple answer is the societal data shows exactly what the trial shows, we were just lied to, primarily through omission, about what the trial showed. How’s that possible you ask, when every single thing you’ve heard says the opposite? Well, let’s break it down…
We have to start by updating the trial death data, because that’s pretty critical. In the original publication, the one I linked too earlier, it showed 29 deaths, with 15 in the “vaccine” arm and 14 in the placebo arm. But… the data presented to the FDA alongside the study to justify FDA approval shows something else entirely — and it was, supposedly, based on exactly the same study, with the same cutoff and evaluation period. Here’s the document: https://www.fda.gov/media/151733/download
On page 23 this document says that “From Dose 1 through the March 13, 2021 data cutoff date, there were a total of 38 deaths, 21 in the COMIRNATY [vaccine] group and 17 in the placebo group.” So, somehow, with the same study over the same period of time, we just went from 15 deaths in the “vaccine” arm to 21, and from 14 deaths in the control arm to 17. Um, what?
I don’t even have a hypothesis, outside of lying, for this discrepancy (the number of covid cases, as a comparison between the study and the FDA authorizing docs, are exactly the same — as they should be). Of course they provide no additional justification, they just state the numbers and move on 10. This is now a greater than 20% gap in mortality rate between the two groups, but the number of “covid deaths” stayed the same. So, by analyzing ONLY covid deaths, Pfizer was able to claim people weren’t dying “of covid” (whatever that means), so the deaths were irrelevant, but at the same time the data CLEARLY shows that all-cause mortality was rising in the “vaccinated” group.
And this makes sense when you think about the data more holistically. Here is the graph above showing death rates by vax status by age group, and here is a general summary of mortality rates by age group, for comparison:
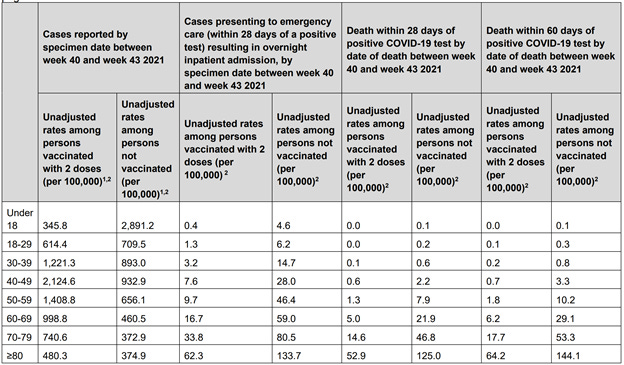
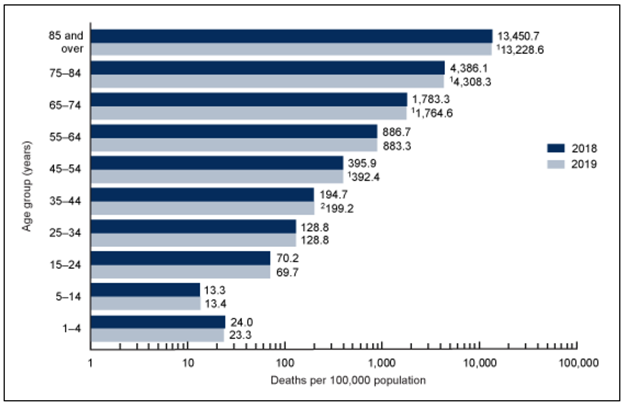
In every single category, the “not-vaccinated” death rates, despite being higher than the “vaccinated” death rates (remember, these rates are ONLY for deaths that are “with” covid), are still SO far below the all-cause base-rate for deaths in that age category, that we really can’t learn anything from this data. We’re talking a death rate of 21.9/100,000 for 60–65 year old's, as compared against an all-cause base rate of 1,783/100,000. This means even in the “unvaccinated,” the “with” covid death rate is less than 2% of total deaths. So, while the data does show a difference in mortality rates, we’re only talking about “covid” mortality which makes up a TINY percentage of all deaths.
When we take a step back and look instead at what is going on with all-cause mortality, well, we see a VERY different story. And it looks something like this:
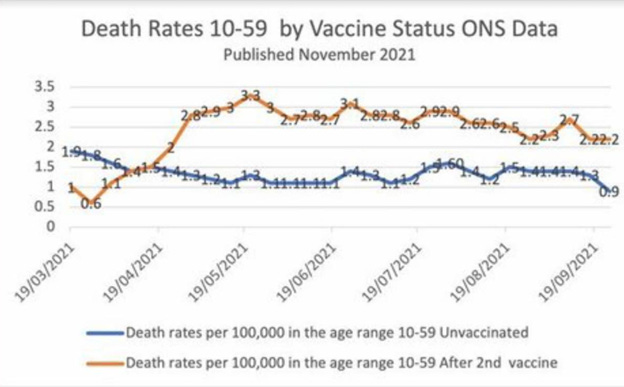
Yes, this chart shows that people who are “vaccinated,” under 60 years of age, are TWICE as likely to die as those that are “unvaccinated.” Now, before you freak out, this data is biased, and we should be honest about that. This shows that you are TWICE as likely to die if you get vaccinated. But that’s not possible. A lot of this is noise created by differences in vax levels by age, and, despite covid-hysterians arguing otherwise, the older you are the more likely you are to die by all causes, and subsequently “with” covid AND the more likely you are to be “vaccinated.” Older “vaccinated” people will always die at a higher rate than younger unvaccinated people and that’s causing a large portion of this illustrated discrepancy. BUT, if you hold constant the ages, you still see a difference, and that difference is in the same range as what the trial showed — somewhere between a 10 and 20% difference in all-cause mortality.
But, you say, covid mortality is down so overall all-cause, across all ages, has to be down meaning the vaccines are working (working was supposed to be eradicating covid, but at this point I guess we’d settle for bringing down all-cause mortality even though we aren’t allowed to talk about all-cause mortality as relates to covid cause then we have to face the Sweden conundrum, and, well, no one wants to do that). But are they actually bringing down all-cause mortality?
I could always point back to Sweden and show that without lockdowns and the removal of basic medical care for the elderly there was no spike in all-cause mortality (you literally can’t correlate covid to all-cause mortality spikes if you look across countries, but you CAN correlate the severity of lockdown to all-cause mortality spikes, as I showed in a piece I wrote last year), but let’s use the UK where there very clearly was a spike in all cause mortality, and take a look. Here is England’s all cause mortality trend for all ages:
As you can see there was very clearly a spike in March of 2020, though it was short lived, and then a relatively prolonged spike in flu season 2021, but it was, at least partially, offset by a decline in March/April in 2021 (this was the impact of bad flu seasons in 2020 and 2018, so “normal” mortality now trended below the line when compared against an elevated base-rate). But now, for the first time in the entire “pandemic,” we are seeing a sustained period of all-cause mortality. Not just spikes, and not normal flu-season, but a summer/fall period of sustained increases in all-cause mortality.
For the same weeks this year vs last year, deaths have risen on an all-cause basis. And keep in mind, these are based on a “base rate” which is constantly changing. 2020’s base rate was based on an EXTREMELY healthy year in 2019, which pulled the base-rate mortality way down. 2021 is based on a base rate of mortality that includes 2020 and therefore should be elevated. So even comparing against an elevated base-rate, 2021 is elevated even higher.
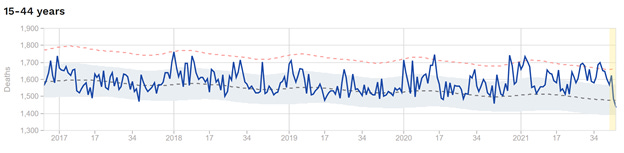
Most concerning to me is this chart:
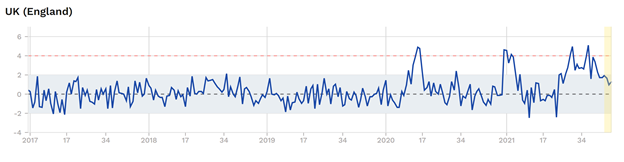
This is ages 15–44. Remember, there was no pandemic for people under the age of 40. Look at the chart above? Tiny spike in March of ’20, tiny spike in December of ’21, but nothing sustained. But now that we’ve introduced “vaccines?” Well, now that we’ve introduced “vaccines,” we’re seeing a sustained increase in all-cause mortality. So not only are we seeing an increase at a macro level, but, significantly more worrying, we’re also seeing increased mortality in a population that DIDN’T see it before.
And that’s exactly what the trial showed. Small numbers for sure, because they left out the elderly (the people who make up the vast majority of deaths), but you can’t hide the data — you were, non-statistically — ~20% more likely to die if you were “vaccinated” than not. And the real-life data is showing exactly the same thing. You may be less likely to be coded to covid (congrats to the dead person for a cleaner death certificate, or something), but the data makes very clear that your chances of dying, regardless of cause, has actually increased thanks to the introduction of these “vaccines.”
But what about covid spread itself? Well, we already know the answer to that, so I won’t harp on it. Again, the trial itself gave us the answer. The efficacy wanes, the Swedish have now released a study showing that after ~9 months, “vaccine” efficacy actually goes negative (meaning you are MORE likely to get covid than if you hadn’t taken the “vaccine”) (10), and that also matches what the societal data shows. Denmark has vaccinated more than 88% of its population (the CDC said we needed 70% “vaccinated” with a 70% efficacy to end this pandemic) and here is their chart of “cases”:
Even talking about these “vaccines” preventing covid, or reducing spread, is, at this point, literally laughable.
And now I’m not even sure where to go from here… I know for sure I don’t like being lied to, but there wasn’t trust left in media or our medical establishment to begin with, and the trial data didn’t actually lie, we just all chose not to read it, and let the media tell us what it said (which is in no way what it actually said) (9), so it’s not like I can really be mad at them. This is par for the course. It was almost a certainty they’d lie with the “future of democracy” hanging in the balance (my goodness) and, much, much, much, much, more importantly, billions and billions and billions of dollars hanging in the balance, which is why I read the study and called bullshit in the first place. But seriously, where do we go from here?
Because my concern isn’t them. Of course they lie. My concern is for us. And for the person who hasn’t yet accepted they’re constantly being lied to. Or maybe the person who doesn’t care the establishment lies? And if you don’t care, that’s fine, it’s your life and you should be free to live it. After all, I argued that “high-risk” should be yours to define. And it should. And similarly, if you want to take medicine that can’t be defended as effective even in its own clinical trials, that is also your prerogative.
But I’m guessing a lot of people didn’t have the information I presented before they made their decision. And it’s unlikely that this really changes people’s minds — I’m assuming at this point you’re pretty firm in your decision but changing your mind on this isn’t really my goal. Shedding light, so maybe you stop, think, and evaluate next time, that’s my goal. I want you to be free to make your decisions and lead your own life, but I’d also prefer we all be informed when we do so.
The life we choose to live
I told someone once the only thing I believe in more than individual liberty is a 2/3rds democracy. If 2/3rds of a population really want to mandate this “vaccine,” they should. That’s what democracy is — a government of the people for the people. More people will die, at this point it’s almost impossible to argue otherwise, but we make democratic decisions not in our own best interest all the time. So, if the people want to mandate “vaccines” to participate in their society, they should. I’d move, just as I did when the schools closed in North Carolina, because that isn’t the society I want to live in, but 2/3rds of people in NC genuinely believed the schools should be closed (because they are constantly lied to), so I didn’t argue. I just found a new community. But for a democracy to function, and for individual liberty to reign, we must have freedom of information. And we must have actual representative government, which mandates are the exact antithesis of. And today, we don’t.
We don’t have to agree on how to interpret the data, or what to do with the data, and some of us will still be manipulated by our emotions, and scared by that one horror story, and ignore the data regardless, and that’s okay. That’s part of what makes democracy wonderful. We shouldn’t have to agree, and we should challenge each other, and hopefully through that become better, but we should HAVE the information. Perhaps I’m preaching to the choir, but perhaps there are people reading this who support suppression of information, and who believe “covid misinformation” is really the threat. Just realize the only people who ever want to limit information are the people lying. Because if you’re being truthful, your information will always win, so why would you care to suppress others?
But that’s a conversation for a different time and place. Today, I just want you to know why I didn’t get “vaccinated,” and why the data says (whether you care for it or not) that I’m less a risk to you as an “unvaccinated” person with natural immunity than any “vaccinated” person is to you, AND I’m less of a risk to myself.
And that’s not emotion, or perception, that’s fact. You should also know that there’s a very good chance you would have been better off “unvaccinated” as well (regardless of age). That doesn’t mean you needed to not take it. I’d be better off if I didn’t speed, but sometimes I’m in a hurry and I trade the tiny increase in risk for the benefit of time. Life is full of tradeoffs. As one very good friend told me when I asked why he got “vaccinated,” “this isn’t even close to the riskiest thing I’ve ever put in my body, and maybe it works.” And he’s right, it probably isn’t the riskiest thing he’s ever put in his body, and maybe it would work… But even he was grasping at straws and hoping for a societal benefit (not being precluded from activities) more than he was expecting any actual health benefit. At the end of the day your risk calculus is (or at least should be) yours, I only hope to consolidate and articulate some data that may be valuable when you make the decisions you make. And to tell you not to be scared of the “unvaccinated,” especially those with actual immunity, the kind earned the way we’ve earned immunity for all of eternity, through our immune system, because that is decidedly irrational.
And finally, to remind you, that with all endemics, this “pandemic” ends whenever you decide it does. And that freedom is pretty great. And that, ironically, exercising that freedom protects you, and I, significantly more than these “vaccines” do.
Zero risk not meaning there is a 0% chance I would die if I got covid. Zero explains the change that covid presents to my baseline chances of dying. This is the importance of understanding base rates (something we have failed MISERABLY at throughout covid). That is, there is a chance I could die with covid, but it is the same as the chance I could die without covid. There is always a chance I could die, covid doesn’t change the odds for someone of my age and health profile.
The biggest farce of covid-19 political/media hysteria is they somehow convinced you that people don’t die. “Even one death is one too many.” This was an actual quote by an actual person actually running for president. “One death is one too many?!?!?!?!” What in the actual hell? I was unaware we were electing God, but then I’m not a democrat (or a republican) so perhaps I just underestimated what the Democrats (capital D, like you capitalize all religions) are actually capable of. Turns out, much to 51% of the country’s surprise, Joe Biden and the Democrats couldn’t actually stop death. But they CAN fix climate change. Seriously, they can. If you don’t believe it, you’re anti-science and a racist or something. Or it’s the “unvaccinated” people’s fault. Or probably both. Either way, it’s DEFINITELY not that they don’t have any idea what they’re doing, but love power. That’s DEFINITELY not it.
This is the best and most complete study to date, and it’s clear about the difference in efficacy between natural immunity and “vaccinated” immunity:
https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.full.pdf — page 12 contains the summary of results
I’d argue it actually understates the benefit of natural immunity, especially over time, because they were comparing during peak “vaccine” protection, which we know wanes significantly over time. If they did this study 9 months after “vaccination,” it’d be a 100x difference, not a 6–13x difference in protection, but either way I believe the point has been established through this study
https://www.vox.com/2018/8/21/17588074/vaccines-diseases-wiped-out — and remember, this is EVER, and when looking at VERY stable families of viruses. The more stable, and the more history we have, the more possible it is to eradicate it. We have a VERY long history with coronaviruses, which is why we know they mutate too quickly to ever be eradicated.
One very important, but always overlooked (purposefully), aspect of our “vaccination” strategy is that we have NEVER vaccinated during a pandemic, because it cannot work. The “public health establishment” argued we hadn’t used that strategy before because we were not advanced enough scientifically to do so — and they were right. Where they were (not shockingly) wrong, is that they wanted to pretend we are advanced enough today. For mass vaccination to work DURING a pandemic, we need not only a perfect vaccine (we’re getting further from this, not closer), but also a PERFECT distribution strategy such that everyone gets exactly the right dose at exactly the right time to protect against exactly the DNA molecule they are coming in contact with. We’re so far away from this reality it’s laughable — and thank God we are, because it’s presented us a perfect real-life comparative analysis showing that countries with very low “vaccination” rates are faring substantially better than their highly “vaccinated” counterparts — because our “perfect” vaccine not only doesn’t work, it makes things worse.
https://www.bloombergquint.com/coronavirus-outbreak/merck-shuts-down-covid-vaccine-program-after-lackluster-data. Merck, the only company to participate in “Operation Warp Speed” (just typing that makes me want to cry) that had actually developed a successful vaccine before, was also, unfortunately, the only one not ready to lie about its data. So it looked at what it had created, realized that targeted antibodies only relevant to one spike protein model were useless, and packed up and moved on. They know you can’t ACTUALLY vaccinate against a coronavirus, so they started immediately working on a treatment. Unironically, Pfizer actually did the same thing — they knew their vaccine wouldn’t work so they immediately started working on a subclass of ivermectin that they could patent and sell. That is what you do when you’re the shadiest medical company in history — the Bear Stearns of medicine, if you will — who has paid the largest medical fraud fine in history; you start working on a treatment at exactly the same time as you’re taking billions to create a vaccine that you already know won’t work… I have VERY little respect for pharma companies, but Merck stands alone in my respect for them. There are great scientists left in the world, and Merck may be the only place left that actually lets them practice science.
https://pubmed.ncbi.nlm.nih.gov/28479213/
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1027511/Vaccine-surveillance-report-week-42.pdf — Dan Wolt on twitter does an awesome job breaking this data down each week and following the surveillance, if you’re interested…
https://www.cnn.com/2020/11/18/health/pfizer-coronavirus-vaccine-safety/index.html
The paper is found here, and the graph is on page 33 — https://poseidon01.ssrn.com/delivery.php?ID=252085073120026109122008077012125086116042064082020028029000097121071083111075017028034036040047022047027073075016120071082084050076003080012025100014118097066006027057010020107081116030068005107091028117100010081089081070116089087123087116127123085100&EXT=pdf&INDEX=TRUE. It shows, after 9 months, a negative efficacy, hypothesized to be due to the specificity of the immune response the mRNA gene therapy creates which actually impacts your ability to then naturally create the broader and more robust immune response even after infection… it also shows significant increases in all-cause mortality rates in the two weeks following vaccination, which I’ll leave you to do with what you please.
Love the steroid metaphor.
MONEY MONEY MONEY MONEY...$$$$$. What a terrific write-up. What I have learned is those who took the vaccine “don’t have the time” (and by that I mean not even 5 minutes) to listen to or read any information that challenges their “knowledge.” And these are otherwise very “smart” and accomplished ppl. Which also means our education system has eradicated critical thinking. And that didn’t happen overnight.